
Prof Salim Abdool Karim Weekly COVID-19 UPDATES
I am writing today’s Epidemic Intelligence missive from Tokyo. Tokyo is the largest city in the world by population – 39million people live in Tokyo! There are more people living in Tokyo than Jakarta, Shanghai or Mumbai.
Regarding the global situation (Figure 1), there were 127,571 (previous week = 141,155) reported Covid-19 cases and 769 (previous week = 927) deaths across the world last Friday. The overall 7-day average number of cases and deaths has dropped substantially from the week before. Such a low number of daily deaths was last seen in mid-March 2020 as the pandemic was still in its infancy then.

In South Africa, the trends in reported cases show no significant changes, under-reporting notwithstanding (Figure 2). The daily number of reported cases remained low overall. Note that 7-day rolling averages are not available as South Africa only reports cases weekly and not daily. XBB.1.5 continues its unchallenged dominance, accounting for most of the viruses sequenced in South Africa last week.

There have been some changes in the source of data as some of the Covid-19 data websites are closing and there is now greater reliance on WHO as the source of data on cases and deaths. Given that the magnitude of the changes week on week are small now, I will be providing these data in the first two slides at the end of the email in future – just so that the more interesting issues are up front.
During this week I spent some time at the WHO Pandemic and Epidemic Intelligence Hub in Berlin. It is an impressive enterprise, though still nascent as it is only in its second year of operation. It has advanced substantially since my last visit to the Hub in September last year – the work streams are taking shape well, the team has been growing and the construction of the building that houses the hub is now almost complete.
This Hub is taking on one of the most important tasks in pandemic preparedness – it is establishing a global early warning network. To do this, the Hub is bringing together national public health agencies to create greater regional synergy and to support these agencies in their crucial role of surveillance for early detection. After all, the best time to stop a pandemic is to “nip it in the bud” early before it spreads geographically to many people. This is easier said than done – but this crucial task, which the WHO has taken up, will help us all sleep a bit easier, knowing that a team of skilled epidemiologists, statisticians and surveillance experts ably led by Chikwe Ihekweazu (leader of the WHO Berlin Hub) have prioritised an early warning network.
The Hub is hosting a meeting with some public health agencies from each WHO region this coming week as part of this initiative – we wish them well. As this is an area that I am keenly interested in, I will occasionally give you updates on this key element of preparing for future pandemics.
Today’s missive deals with a question I was asked following my plenary address at the Canadian Covid-19 Immunity Task Force meeting last Wednesday – Is Long Covid more common in those who had clinical Covid-19 infection compared to those who had mild or asymptomatic infection? Since this is a national Canadian network of investigators conducting serological studies, the question as it relates to them is whether those who are identified only serologically as having been infected are also at risk of Long Covid and how does this risk compare to those diagnosed with clinical illness.
In Figure 3 below, I summarised some of the studies to illustrate the trend in the data. Most studies show that Long Covid-19 occurs in those who only had asymptomatic infection and it appears that the rates in this group are not too different from the rates in those who had clinical infection. However, the caveat is severe infection. Those who had severe Covid-19 – many symptoms/signs or needed oxygen supplementation – have a much higher risk of Long Covid.

- Avoid getting infected at all or getting repeat infections. Primary prevention of infection is the surest way of reducing the risk of Long Covid.
- Get vaccinated! If a vaccinated person gets infected, the risk of Long Covid is 34% lower than in unvaccinated people. (Figure 4)
- But getting infected or re-infected has a component of the risk that is outside your own control. For those who get infected clinically and are diagnosed with Covid-19, taking Paxlovid has been shown to reduce the risk of developing Long Covid. (Figure 5)
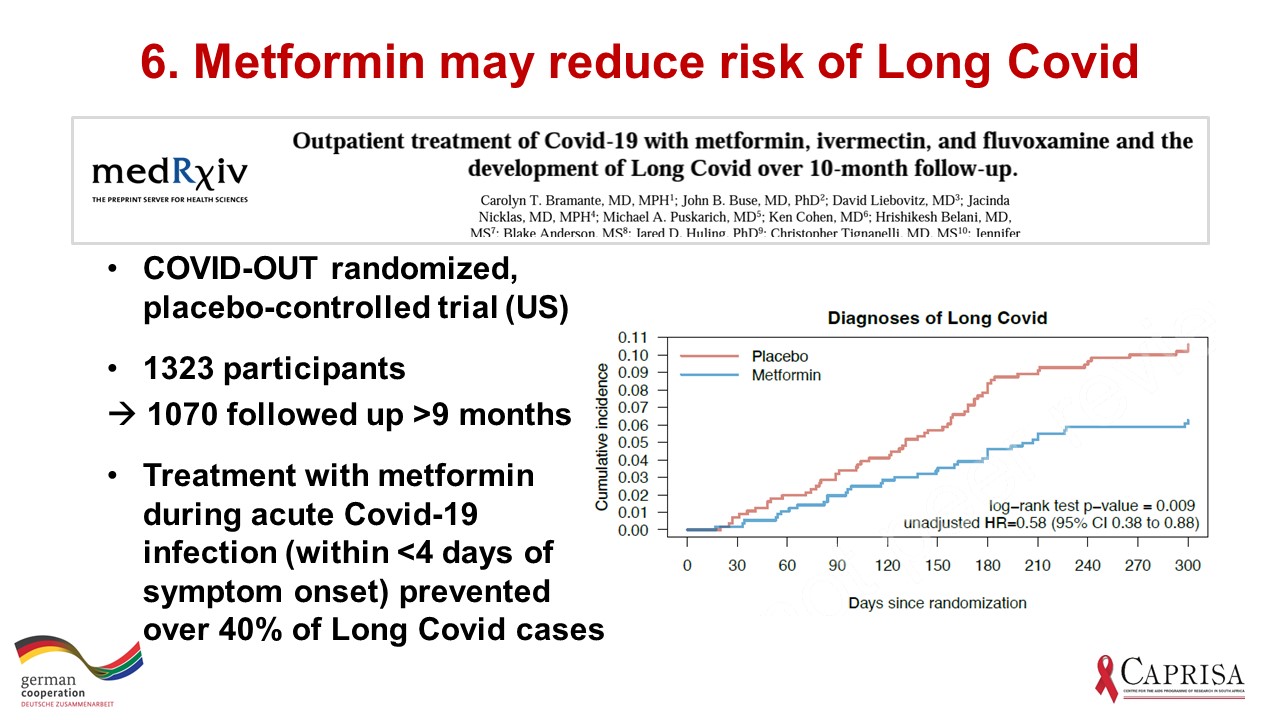
- And a pre-print just out, which has not been peer-reviewed, suggests that Metformin, a widely used treatment for Type 2 diabetes, may reduce the risk of Long Covid. (Figure 6)

The data showing a 34% reduction in Long Covid in those with 2 vaccine doses compared to unvaccinated comes from a meta-analysis of 6 longitudinal studies (Figure 4). I am not sure what to make of the observation that if an unvaccinated person gets Long Covid, getting vaccinated seems to reduce the symptoms severity by 20% (Figure 4). I am waiting for corroborating evidence before promoting this idea.
Paxlovid reduces Long Covid by 26%, in addition to reducing progression to severe disease (Figure 5) – this is from real world experience in VA.

I was a bit surprised by the Metformin data showing a reduction in Long Covid since the primary outcome of the Metformin trial published by this same team in the NEJM showed no benefit of Metformin in reducing severe disease (Figure 6). I will wait for corroborating data on this
So, remember that there is a lot you can do to reduce your risk of Long Covid, including interventions that are effective when taken after a Covid-19 infection has been diagnosed.
Have a great week
Yours